
1Department of Rehabilitation Medicine, Danderyd University Hospital, and 2Department of Clinical Sciences, Division of Rehabilitation Medicine, Karolinska Institutet, Danderyd Hospital, Stockholm, Sweden
Objective: To explore whether the use of personally relevant stimuli, for some tasks in the Coma Recovery Scale – Revised (CRS-R), generates more responses in patients with prolonged disorders of consciousness compared with neutral stimuli.
Design: Multiple single-case design.
Subjects: Three patients with prolonged disorders of consciousness recruited from an inpatient department at a regional brain injury rehabilitation clinic in Stockholm, Sweden.
Methods: Patients were repeatedly assessed with the CRS-R. Randomization tests (bootstrapping) were used to compare the number of responses generated by personally relevant and neutral stimuli on 5 items in the CRS-R.
Results: Compared with neutral stimuli, photographs of relatives generated significantly more visual fixations. A mirror generated visual pursuit to a significantly greater extent than other self-relevant stimuli. On other items, no significant differences between neutral and personally relevant stimuli were seen.
Conclusion: Personally relevant visual stimuli may minimize the risk of missing visual fixation, compared with the neutral stimuli used in the current gold standard behavioural assessment measure (CRS-R). However, due to the single-subject design this conclusion is tentative and more research is needed.
Key words: consciousness disorders; minimally consciousness state; vegetative state; unresponsive wakefulness syndrome; personally relevant stimuli.
Accepted Nov 24, 2017; Epub ahead of print Jan 9, 2018
J Rehabil Med 2018; 50: 00–00
Correspondence address: Jonas Stenberg, Danderyds sjukhus AB, Rehabiliteringsmedicinska Universitetskliniken, SE-182 20 Danderyd, Sweden. E-mail: jonas.stenberg@ntnu.no
Patients with a severe acquired brain injury usually emerge from coma and gradually regain a greater or lesser degree of independence. A small group of patients, however, open their eyes but show no or extremely limited signs of consciousness, and are described as having a disorder of consciousness (DOC). Prolonged DOC (PDOC) (≥ 4 weeks) encompasses unresponsive wakefulness syndrome (UWS, previously called vegetative state) (1), where patients show no behavioural signs of consciousness, and minimally conscious state (MCS) where patients show “clearly discernible”, but inconsistent, signs of consciousness (2). Emergence from MCS is marked by the emergence of functional communication and/or functional object use (3). PDOC is uncommon, the annual incidence of DOC after traumatic brain injury persisting for at least 3 months is estimated to be less than 10 per million adults per year (4, 5). The prevalence of UWS is estimated to be between 2 and 61 (6, 7), and for MCS approximately 15 (7), cases per million inhabitants. Patients with MCS generally have a better prognosis than those with UWS (8, 9) and it is thus of clinical and ethical relevance to distinguish between these states. However, even within these categories, there is a considerable spectrum of conscious level, and it seems likely that prognosis is different for patients at the upper and lower ends of “UWS” and “MCS”, respectively. The proposed subcategorization of MCS in MCS+ and MCS– (10) has attempted to address this. Recently, it has been argued that consciousness is better understood on a continuum (11). Whichever view is taken, the clinical challenge is to use methods that give the greatest likelihood of capturing any conscious responses.
Assessing a patient’s level of consciousness is challenging, but the use of standardized behavioural scales enhances the sensitivity of the assessment (12). The Coma Recovery Scale – Revised (CRS-R) is the recommended behavioural scale to use when standardization of administration, validity and reliability are under consideration (13). Although the CRS-R is the recommended scale it has limitations. Several studies have shown that some patients who, according to results from behavioural-based assessments are in UWS, in fact have brain activity that indicates consciousness, when neuroimaging and electrophysiological methods are used. A meta-analysis concluded that 15% of the patients who, according to behavioural scales, are unresponsive, show signs of consciousness when assessed with functional magnetic resonance imaging (fMRI) or electroencephalography (EEG) (14). However, in addition to not always being practically feasible in the clinical setting, these methods are not precise enough to be used in clinical practice today (15, 16), the frequency of false positives is difficult to estimate due to the absence of a gold standard in assessing consciousness (14), and false negatives may also occur. Irrespective of this, studies have shown that a subgroup of patients with PDOC probably have a higher degree of consciousness than detected with behavioural-based assessment. Thus, the behavioural scales have limitations that should be addressed.
Personally relevant stimuli are not used during assessment with the CRS-R. This despite research indicating that the use of personally relevant stimuli, compared with neutral stimuli, elicits a higher frequency of responses. Research on patients with PDOC has shown that photographs of relatives elicit more responses compared with neutral stimuli (17, 18); that patients more clearly react to their own name compared with neutral sounds (19); that patients to a greater extent follow their own reflection in a mirror than neutral stimuli (20, 21); and that more responses are seen when meaningful stimuli are used during assessment (22). In clinical practice, there is a need to use personally relevant stimuli during assessment of consciousness in a standardized way; however, this has not been systematically studied. A relevant reaction to emotional or personally relevant stimuli may demonstrate a higher degree of consciousness and, as such, this is relevant for prognosis as well as future rehabilitation.
The aim of this multiple single-case study is to explore whether the use of personally relevant stimuli, for some tasks in the CRS-R, generates more responses in patients with PDOC compared with neutral stimuli. We hypothesized that personally relevant stimuli would generate significantly more responses.
Patients were recruited from the regional specialized rehabilitation department at Danderyd Hospital, Stockholm, Sweden. Recruitment occurred between September 2016 and June 2017 and all patients with suspected PDOC (based on information in the referral letter and the initial clinical assessment by the rehabilitation specialist at the hospital) referred to the clinic in the recruitment period were considered for inclusion. The inclusion criteria were: admission to the clinic; suspected PDOC after acquired brain injury of various aetiologies; and assent from relatives. Exclusion criteria were: the criteria for a PDOC diagnosis were not fulfilled after 2 assessments with CRS-R; and suspected cortical blindness according to visual evoked potentials and 0 points on the visual subscale in CRS-R during the first 2 assessments. Cortical blindness was judged to be an essential exclusion criterion because 4/5 of the items listed below require near normal vision. One patient was excluded due to cortical blindness. Because 2/5 items (Fixation and Visual Pursuit) can be administered independently of hearing loss/deafness, it was decided not to include this as an exclusion criterion.
Four patients with suspected PDOC were admitted to the clinic during the recruitment period, 3 were included in the study (Table I). All of them fulfilled the criteria for MCS after 2 assessments with CRS-R.
Table I. Characteristics of included patients
An authorized, back-translated, Swedish version, of the original CRS-R (23) was used. The validity of the Swedish translation is based on the validity of the Norwegian translation (24), the 2 languages being closely related and largely inter-intelligible. CRS-R is a standardized scale used for the assessment of consciousness. In an evidence-based review, the CRS-R was the only scale recommended for use with only minor reservations, with good inter-rater reliability and content validity judged to be excellent (13). The internal construct validity of the scale has been confirmed with Rasch analysis (25). The scale consists of 6 subscales and each of the subscales consists of several items. Each item has specific scoring criteria. E.g. for the item “fixation” in the visual subscale, at least 2 fixations (out of 4 trials) with a duration of 2 s must be observed to achieve the score for visual fixation.
Each patient was scheduled for 10 assessments with the CRS-R during a period of 3 weeks. No more than one assessment per day was performed. Repeated assessments are recommended because the level of consciousness, wakefulness and general condition fluctuates in patients with PDOC. Due to these factors, 10 complete assessments could not be performed with each patient; the tables in the results section show how many items were performed. JS conducted all but 2 assessments. A second psychologist (IEM or MH), otherwise not involved in the study, was also present during the assessments. CRS-R was scored in consensus according to the manual. IEM conducted the 2 assessments not conducted by JS. JS and IEM had previous experience with the patient group and with CRS-R. All assessors read the manual thoroughly and watched the instruction video before the study started.
Immediately before or after the assessments with CRS-R 5 items from the scale were administered with personally relevant stimuli. This administration followed the same standardization and criteria as in the CRS-R proper, except that the stimuli used were personally relevant to the patient. To avoid presenting order effects (e.g. due to fatigue), these items were alternately presented before or after the assessment with CRS-R, as illustrated in Fig. 1.
Fig. 1. Design of the assessments. Every patient was scheduled for 10 assessments. Five items with personally relevant stimuli were alternately presented before or after assessment with the Coma Recovery Scale – Revised (CRS-R).
When relatives were invited to assent to the study, a short structured interview (approximately 20 min) was conducted to determine what kinds of personally relevant stimuli should be used. The relatives were asked to bring 2 photographs of relatives or friends and 2 personally relevant objects. Objects finally used were: ornaments, teddy, video game cover, tea-cup, cap, and coffee cup. All objects used were from the patients’ home environment.
Because patients with PDOC often have reduced arousal and have major attention problems when awake, not all of the CRS-R items were administrated with every stimulus. To keep the assessments short, and thereby minimize the risk of patients falling asleep, a specific kind of stimulus was prioritized for a specific item. The 5 items and the stimuli used are described below.
Object-related eye movement commands (auditory function scale). Two objects were presented. The patient was asked to look at one of them in a total of 4 trials. To score the item, 4 accurate responses must be observed within 10 s. Thus, 0–4 correct visual fixations can be observed in this item. The CRS-R administration guide states that “two common” objects should be used; in this study a comb and a plastic apple were used. This item was the only one in which all 3 kinds of stimuli were administered: neutral, photographs of relatives and personally relevant objects.
Localization to sound (auditory function scale). A sound was presented from the patient’s left and right sides in a total of 4 trials. To score the item, head or eyes must orient toward the sound on both trials in at least one direction. Thus, in this item 0–4 correct localizations can be observed. The administration guide states that auditory stimuli, such as a voice or noise, should be used. In the present study a can, filled with small objects and shaken, was used as the neutral stimulus. As a personally relevant stimulus the subject’s own name (SON) was used.
Object localization: reaching (visual function scale). An object is presented on the patient’s left and right sides in a total of 4 trials. The patient is encouraged to reach for the object. To score the item, the first move of the limb must be in the correct direction in 3/4 trials. Thus, in this item 0–4 correct localizations can be observed. The administration guide states that a common activities of daily living (ADL) object should be used. In this study a comb was used, or if the function was better in the lower extremities, a ball. As a personally relevant stimulus, a personally relevant object was used.
Visual pursuit (visual function scale). A mirror is held in front of the patient’s face. It is moved twice in the vertical midplane and twice in the horizontal plane. To score the item, the eyes must follow the mirror without loss of fixation for 45° on 2 occasions. In order to quantify this for the purposes of the present study, 45° represented 1 point, hence 0–8 points could be scored in this item. This quantification has been used in earlier studies of patients with PDOC (26). This is the only item in the CRS-R where a self-relevant stimulus is already used (the reflection of the patient’s own face). The item was also administered with a personally relevant object.
Fixation (visual function scale). An object is presented in the patient’s upper, lower, left and right visual field. To achieve the score for visual fixation item, the target must be fixated for at least 2 s, on 2 occasions. Thus, 0–4 fixations can be observed. In the administration guide it is stated that a brightly coloured or illuminated object should be used. In this study a bright purple ball was used as a neutral stimulus. As a personally relevant stimulus a photograph of a relative was used. Patient 1 was assessed with a personally relevant object. The study protocol was adjusted after this patient in order to balance between the number of assessments with a personally relevant object and a photograph. Patient 1 is therefore excluded from the analysis of this item. During the first 6 assessments patient 2 was presented with the stimulus 16 times, instead of 4. However, only the first 4 presentations were scored and analysed.
With only 3 participants, group level analyses were not possible. However, because every patient was assessed repeatedly, statistical analysis was possible at the individual level. For every patient and item, approximately 10 assessments with neutral stimuli and 10 with personally relevant stimuli could be analysed for significant differences. Testing for significant differences across patients was not suitable considering the mix of dependent and independent observations, because every patient was assessed repeatedly.
Randomization tests (also called re-sampling test, permutation test, bootstrapping) were used to test for significant differences in number of responses when neutral and personally relevant stimuli were used. Randomization tests are a non-parametric method often recommended for single-case analysis (27). No assumptions of the underlying population are made when using randomization tests; instead the observed data is shuffled repeatedly to calculate the probability of the null hypothesis being true, or in other words, the probability of a difference as large as the observed occurring by chance. A total of 50,000 randomizations were conducted for each analysis. The p-value was calculated by counting the number of times the difference was as large, or larger than, the observed.
Spearman’s rank correlation was used to explore the correlation between total CRS-R score and the chronological number of the assessment for each patient, indicating whether the patient performed increasingly better.
Alpha 0.05 was applied (2-tailed). However, multiple statistical analyses were performed in the study, which enhances the risk of type 1 errors. A typical Bonferroni correction is often regarded as too conservative; therefore the significance level was adjusted with the Bonferroni-Holm method (28).
Data were handled with IBM SPSS Statistics 22 for Windows (IBM Corp., Armonk, NY, USA). Analyses were performed with SPSS, except for the randomizations tests, which were performed in Excel 2016 for Windows (Microsoft Corp., Redmond, WA, USA) with the add-in “Excel add-in v 4.0” (http://www.resample.com/excel/).
Patients with suspected PDOC are, by definition, unable to give informed consent. The patient’s nearest relatives received written information on the study and gave written assent. The study was approved by the regional ethics committee in Stockholm (2016/1195-31/1).
Fig. 2 shows the CRS-R total score for each patient and each assessment. The Spearman’s rank correlations between the total score and the point of assessment (1–10) were positive, indicating that the patients performed increasingly better on CRS-R. For patient 1, r = 0.86, patient 2, r = 0.63, and patient 3, r = 0.26. The correlation was significant for patient 1 (p = 0.003).
Fig. 2. Coma Recovery Scale – Revised (CRS-R) total score (min 0, max 23) for each assessment and each patient. The y-axis shows CRS-R total score and the x-axis shows the assessment number in chronological order.
Table II shows the results from the items that were administered with both neutral and personally relevant stimuli. Regarding the item “object-related eye movement commands”, the differences in response frequency when using neutral stimuli, photographs of relatives, and personally relevant objects, were non-significant for all patients. Regarding the item “localization to sound”, the differences in response frequency when using neutral sound and the subject’s own name were non-significant for all patients. Regarding the item “object localization: reaching”, the differences in response frequency when using neutral object and personally relevant object were non-significant for all patients. Regarding the item “visual pursuit”, the mirror generated significantly more responses than a personally relevant object for patient 2 (p = 0.0002, α according to Bonferroni-Holm 0.0033). The mirror also generated more responses for patient 3, but the difference was not significant after correcting with Bonferroni-Holm (p = 0.026, α = 0.0038). No significant difference was noted for patient 1. According to the instructions in the CRS-R, this item can only be scored if a minimum of 2 visual pursuits of at least 45° are seen. For patient 2, this criterion was fulfilled in 90% (9/10) of the trials when the mirror was used, and in 30% (3/10) of the trials when the personally relevant object was used. In Table III, the number of fulfilled (scoring criteria met) and administered items for every stimuli condition and every assessment, across patients, are seen. Regarding “visual pursuit”, for all the patients, 60 trials were administered; 30 with a mirror as stimulus and 30 with a personally relevant object. When the mirror was used the criteria was met in 80% (24/30) of the trials and when a personally relevant object was used it was met in 33% (10/30) of the trials. Regarding the item “fixation”, photographs of relatives generated significantly more responses than a neutral stimulus for patient 2 (p = 0.001, α according to Bonferroni-Holm 0.0036). No significant difference was noted for patient 3. According to the instructions in CRS-R, this item can be scored when a minimum of 2 fixations with a duration of at least 2 s are observed. For patient 2, this criterion was fulfilled in 100% (9/9) of the trials when photographs of relatives were used, and in 56% (5/9) of the trials when a neutral stimulus was used. For both of these patients, a total of 38 trials were administered; 19 with a photograph of a relative as stimulus and 19 with a neutral stimulus. When using a photograph of a relative, the criterion was met in 53% (10/19) of the trials, and when using a neutral stimulus, the criterion was met in 26% (5/19) of the trials (Table III).
Table II. Results from the items administered with neutral and personally relevant stimuli
Table III. Number of fulfilled and administered items for every stimuli condition across patients
The present study explored whether the use of personally relevant stimuli generated more frequent responses demonstrating consciousness in patients with PDOC, compared with neutral stimuli. For one patient, photographs of relatives led to more fixations than did neutral stimuli. The patient’s own reflection in a mirror was a self-relevant stimulus that generated visual pursuit to a greater extent than did another personally relevant object. For the other items in the CRS-R no significant differences between personally relevant and neutral stimuli were found.
That the reflection in a mirror has greater potential than other objects in generating visual pursuit in patients with PDOC has also been seen in earlier studies (20). However, to the best of the author’s knowledge, no earlier study has compared the mirror with another self-relevant stimulus, as was done in the present study. Cruse and colleagues (29) used eye-tracking technology to examine why the mirror was superior and found that the mirror generates shorter fixations than other objects. The authors argue that this gives a smoother pursuit that is easier for the assessor to detect.
In the present study, the use of photographs of relatives as stimuli generated significantly more fixations for patient 2 on the item with the same name, than did neutral stimuli. The same result has been found in earlier studies (17, 18).
The authors of the present study are not aware of any other study that has compared the number of responses generated by different stimuli on the items “object-related eye movement” and “object localization: reaching”. As earlier stated, no significant differences in the number of responses were noted on these items. “Object-related eye movement” is one of the most demanding items in the CRS-R, requiring that the patient both sees and can interpret what is seen, hear, and understand a verbal command, and finally has the ability to execute the command. It is possible that, due to this complexity, the type of stimuli used is secondary. Hence, if the task is too complex for the patient to perform it does not matter if the stimuli are interesting. However, this is speculative, the small sample size and limited power make it difficult to reach a firm conclusion regarding this negative finding.
On the item “object localization: reaching” there was a tendency toward more numerous responses for the non-personally relevant object, especially for patient 2. In this item the patient is encouraged to reach (if the best function is in the upper extremities) or kick (if the lower extremities have the better function), patient 2 was encouraged to kick. It is possible that a ball, due to the nature of the object, has greater potential to generate kick movements than another object, even if this object is personally relevant. It could be that the degree of personal relevance is secondary to how natural it is to reach for, or kick towards, the object in question.
Photographs of relatives led to emotional responses for patient 1. During 3 out of 10 assessments the patient started crying. Even though this did not generate points on the item (object-related eye movement) it provided important information about the patient’s level of consciousness. The fact that it is not possible to score emotional responses is a limitation with the CRS-R, especially when situationally appropriate emotional responses can differentiate between UWS and MCS. This limitation becomes most evident when emotional and personally relevant stimuli are used.
Regarding the item “localization to sound”, no significant differences in the number of responses were noted when a neutral sound or the SON were used as stimuli. This was surprising; an earlier study (n = 86) found that SON generated more numerous responses than a neutral sound (19). However, in that study the duration of the neutral sound and the SON was the same. According to the instructions in the CRS-R the stimuli should be presented for a period of 5 s. Thus the SON must be repeated several times; however, in the present study it was only presented once. This could explain the difference in results between the studies. Even though the SON did not generate more points on the item, for patient 2 it generated verbal responses not generated by neutral stimuli. On one occasion the patient answered “What do you want?”. Similarly to the item “object-related eye movement”, the use of personally relevant stimuli provided important information about the patient’s level of consciousness, without generating points on the item in focus. The response indicates that the patient was on his way out of MCS. In this specific case, personally relevant stimuli were helpful in the differentiation of the proposed subdivision of MCS in MCS+ and MCS– (10), and in the differentiation between MCS and emergence from MCS. However, the scoring procedure did not allow this response to be scored, which could be considered as a limitation of CRS-R.
All patients in this study performed increasingly better on the CRS-R during the course of the study, indicating that recovery was ongoing. This is not surprising, given that the time between injury and first assessment was relatively short (7–11 weeks). However, because the stimuli used, both personally relevant and neutral, were continuously alternated, recovery should not have affected the results.
First, with only 3 subjects it is not appropriate to generalize these results to all PDOC patients. Data were analysed on an individual level with randomization tests; therefore a significant result is significant for only that individual, the probability that the difference exists in the PDOC population cannot be estimated. However, PDOC is rare and many studies include only a few subjects. The results from these, including the present study, must be interpreted in a broader clinical and research practice. Also, the assessors were not blind to the hypothesis of the study. This, of course, may have affected the results. However, due to the nature of the study, blinding is extremely difficult. Furthermore, it is known that the neural processing of faces is different from other visual processing (30). It is possible that faces generate more numerous responses in patients with PDOC, no matter whether the faces are familiar. The argument for not including a photograph of an unknown face as a control in the present study is the same as for not administering all kinds of stimuli on all items: the assessments must be as short as possible to minimize the risk of inattention and fatigue. Finally, no UWS patients were admitted to the clinic during the time of inclusion. Therefore, it was not possible to analyse whether the use of personally relevant stimuli had the potential to better differentiate between MCS and UWS. This potential has been shown in an earlier, small, study on patients with PDOC (17).
The results of the present study, together with earlier research in the field, indicate that, in some cases, personally relevant, compared with neutral, stimuli have the potential to generate more responses in patients with PDOC. In some cases these additional responses are sufficient to diagnose the patient with a higher degree of consciousness. Because diagnosis and degree of consciousness have consequences for prognosis and rehabilitation planning, this is important information for clinicians and relatives. When assessing patients with PDOC, using stimuli with the greatest potential to generate responses is an ethical, time- and cost-effective way of enhancing the sensitivity of the assessment. However, more research is needed before a conclusion can be drawn regarding what type of stimuli, for which items, have the greatest potential to generate responses. The present study indicates that the type of stimuli, e.g. the degree of personal relevance, is of greater importance for some items than for others. It is also possible that personally relevant stimuli have greater potential in discriminating between different levels of MCS, or between MCS and emergence from MCS, than between UWS and MCS. In support of this; the significant differences found in the present study, were found in the patient with the overall highest total CRS-R score (Fig. 2). This is a question for future studies to explore further. Larger sample sizes are needed to answer these questions, therefore, multicentre studies are recommended.
The assessment of visual fixation in severely brain-damaged patients is challenging. Lately, a few studies on patients with PDOC have started using eye-tracking technology to add objectivity (18, 26, 31). This technology allows precise measures of frequency and durations of visual fixations. To avoid the uncertainty following the judgements of clinicians and researchers, this technology will probably become more used in the future. The technology also makes lack of blinding less of a problem.
In the present study, personally relevant stimuli generated emotional reactions for one of the patients. These reactions are not scored in CRS-R, but nevertheless can indicate a higher degree of consciousness if situationally appropriate and reproducible. It can be argued that the development and inclusion of an “emotional subscale” in CRS-R would improve the scale.
To summarize, a tentative conclusion from the present study is that photographs of relatives have great potential for generating visual fixations, and a mirror has great potential for generating visual pursuit. It is likely that the degree of personal relevance is of less importance for some items. It might be that the type of stimuli is secondary in more complex items. In other items, it is possibly more important that the stimulus used is relevant in the setting, rather than being of personal relevance. However, due to the small sample size, the negative findings in the present study should be interpreted with caution. Finally, personally relevant stimuli have the potential of generating emotional responses that are not scorable in the CRS-R, therefore the inclusion of an emotional subscale would improve the scale.
The authors thank psychologists Iina Ervamaa Mekahal (IEM) and Martin Hemmingsson (MH) for assistance with the assessments, the patients and their relatives.
Funding. This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize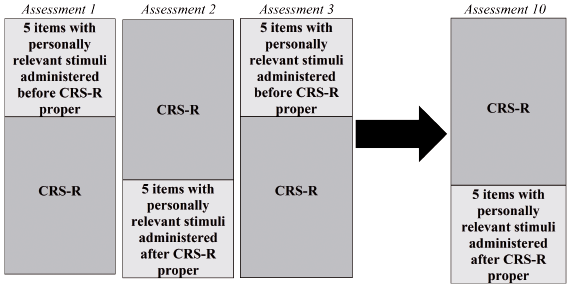 Click to show fullsize
Click to show fullsize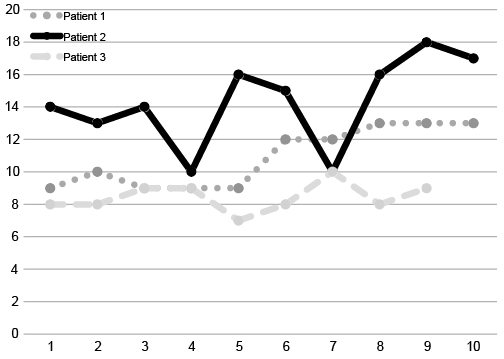 Click to show fullsize
Click to show fullsize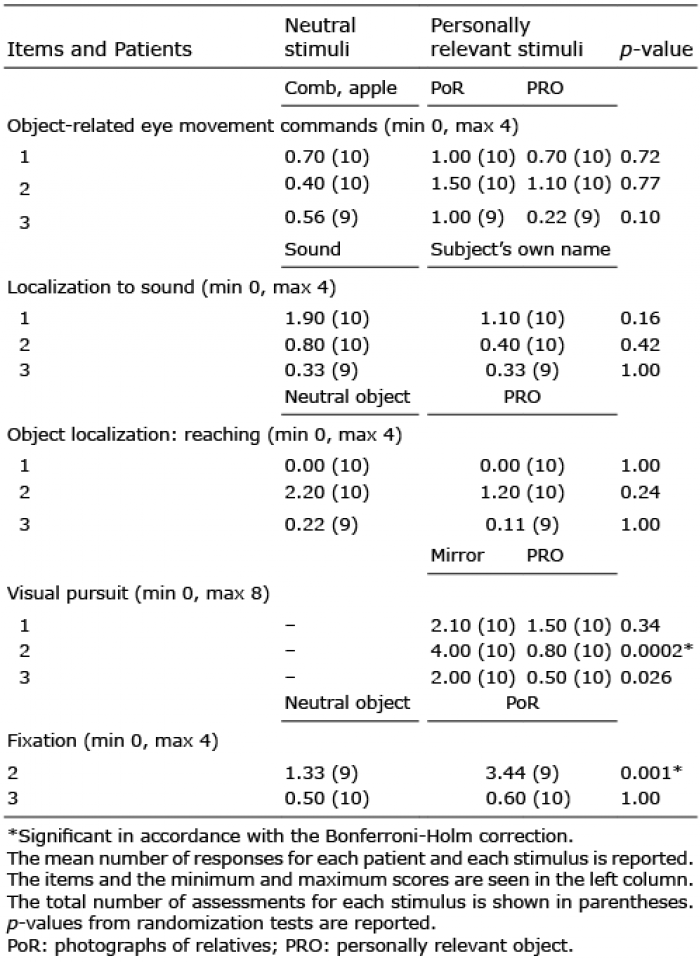 Click to show fullsize
Click to show fullsize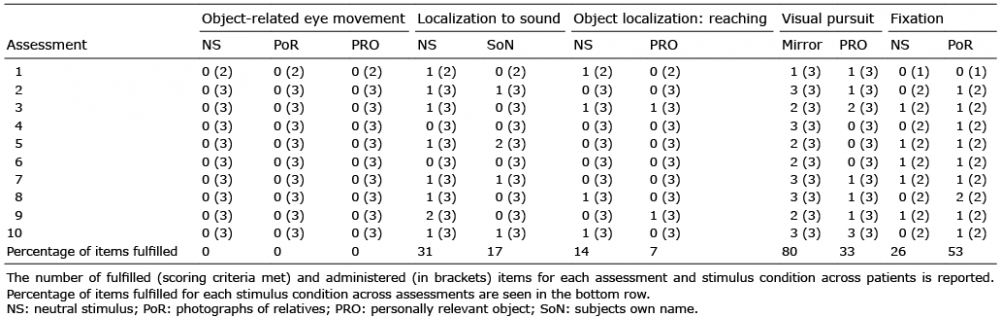 Click to show fullsize
Click to show fullsize